EBD speaker – Communications Manager
Main points:
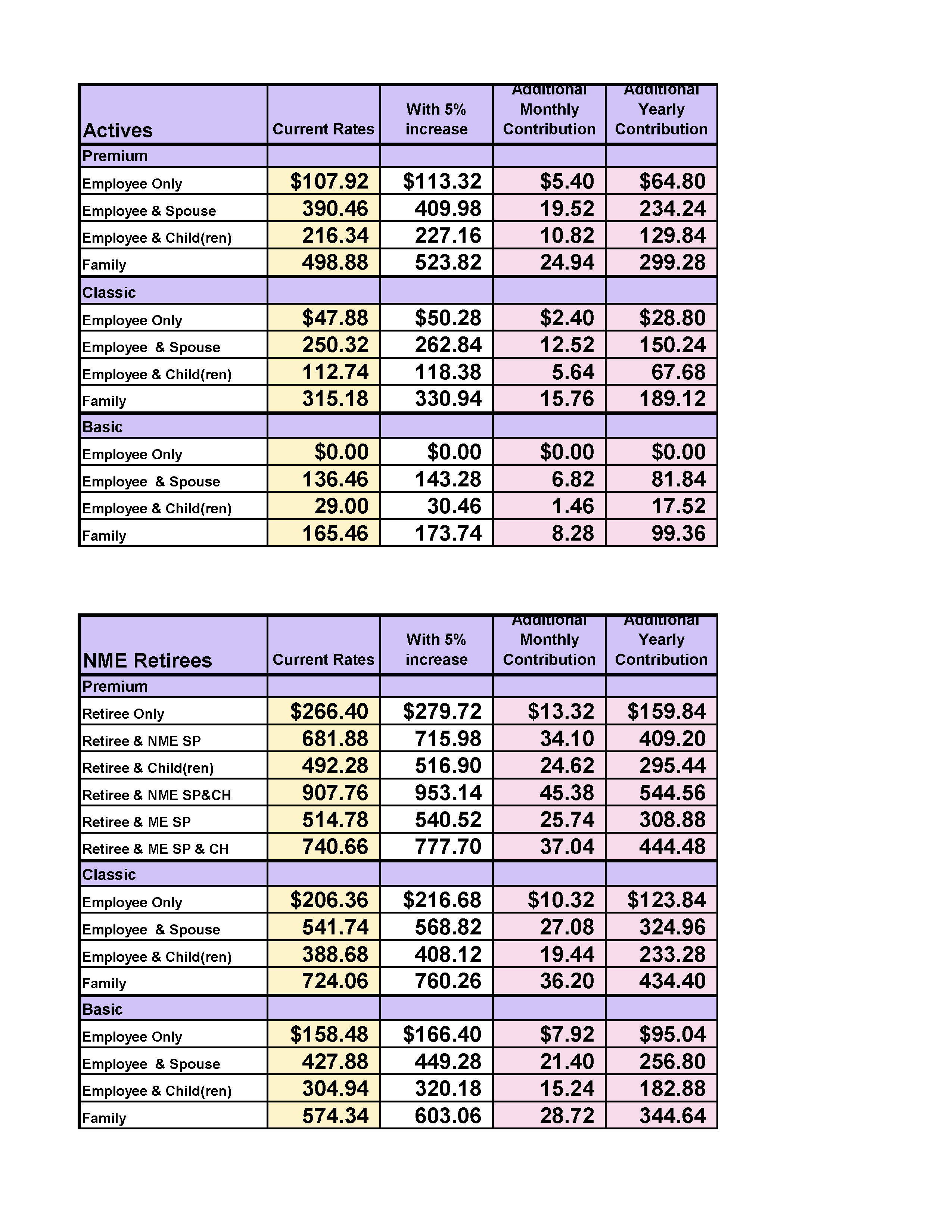
- In March the actuaries estimated there would be $27 million that needed to be made up by the end of 2020 to break even.
- If all was put on the members, it would have been a 27% rate increase. The board decided against that as it “would be a total disaster”.
- What can the plan do? Looked at four options:
- What if active employees rates the agency contributes goes up? (That’s more for DF&A to decide, not an option).
- What if on state employee premium plan, matched deductibles to what PSE side had? Non-Medicare premium $500 deductible, if anyone else covered, $1,000 deductible. School side, $750 for individual and $1,500 for family. Would save $4 million.
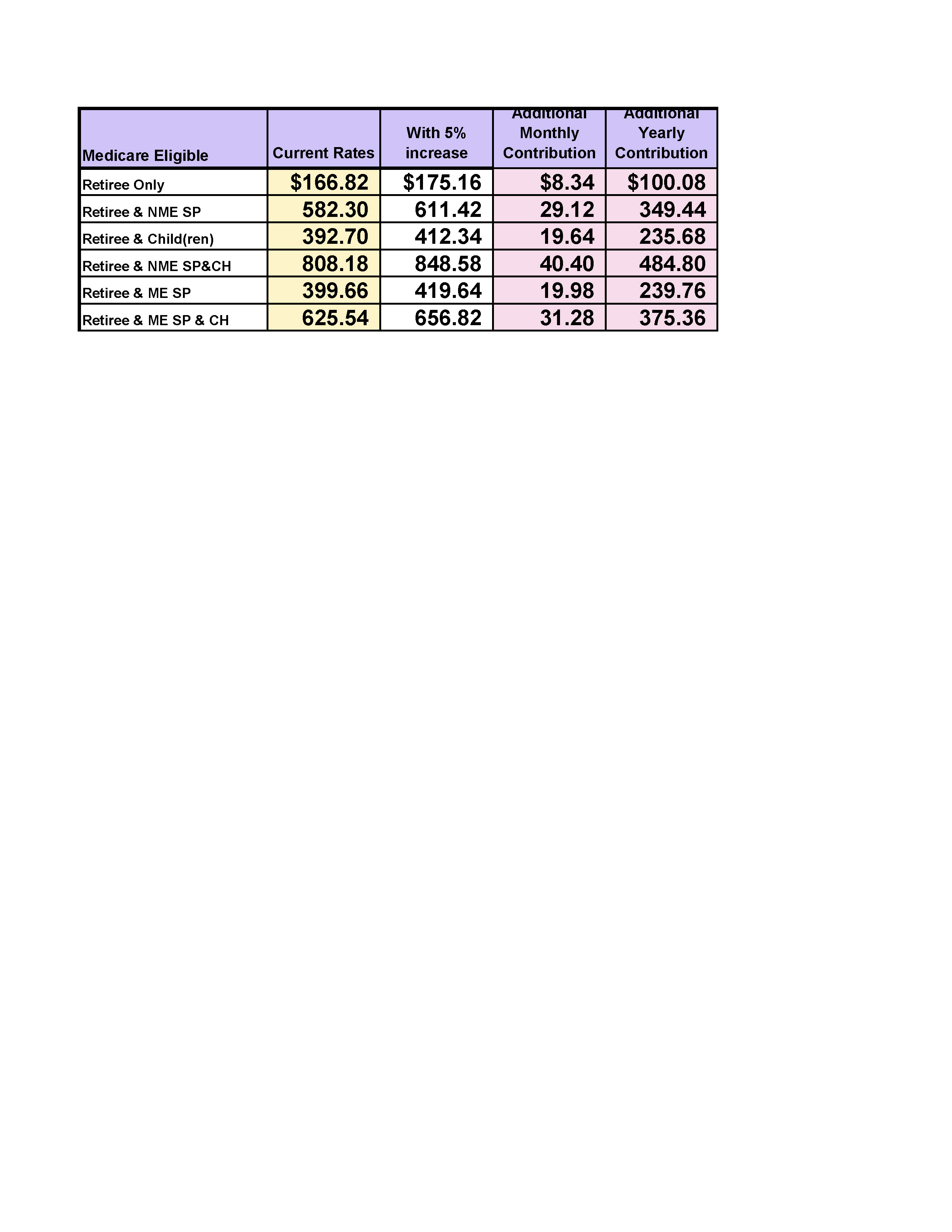
- Medicare Part D approach? Premiums would decrease, $20 million saved a year if no drug plan.
Pros – saving $20 million a year, could prevent future rate increases. Cons – getting all retires to be informed, when and what etc. Membership side, pros – premium goes down. Would have to get part D for Rx coverages. Would have some negative affects – some drugs may not be covered.
- All this was provided as informational purposes in meetings to board only.
- Meeting last month, late May, numbers down to 16% rate increase if all on members. If deductible plan, 12%.
- Meeting is 6/14/19 at 10:00 a.m.; will know more after that. Everyone is welcomed to come. ASEA will shuttle again as usual.
Q&A:
Q – Medicare eligibility and late fee if not taking part D?
A – You have an edibility window for Medicare, if on our plan now, you don’t need part D, we get a subsidy, so if you get part D, that subsidy stops. If board does part D change, and you’re out of your enrollment window? You’d be losing credible drug coverage through the plan, and that would open up a special window to enroll without penalty. We send out COCC’s to everyone, you can give to Medicare and it can open up that window.
Q – How much cost for Medicare Part D for same coverages we have now?
A – Part D is more privatized, can have through several companies, depending on meds, can be anywhere from $20 – $90/month.
Part D can be expensive and about 20% could be affected in a negative way if we went that way and that’s why the drugs matter and type of plan etc. Hopefully it doesn’t come to that.
Director spoke at last board meeting, this isn’t all a recommendation at all, we know it would be a really tough plan to put into place. The 2015-2017 claims were really low, especially on Rx side, we weren’t getting multi-million-dollar claims, but now that has picked up as of last year.
Q – Does the state pay part of Part D?
A – No, your premium includes drug coverage through the state, pharmacy and medical are included in your medical. If you have secondary coverage that includes that pharmacy coverage.
The board hasn’t discussed any changes to the plan benefits wise for active employees or non-Medicare retirees, but your rates will likely go up next year possibly. Non-Medicare retirees, not taking Rx away from them.
Q – Has anyone suggested making it optional?
A – That was one of the things discussed as far as taking the drug plan with us or not, the board looked at that too, if we could do a Medicare plan with drugs or without and we weren’t sure if it would be able to be administrated through EBD and how that would affect subsidy. If we split, would that go away? Subsidy amount is a significant amount we get reimbursed for. If no subsidy, how do you make up for the loss of that money? If we don’t have drug program, don’t need subsidy funds anymore.
Q – Advantage plan, same subsidies?
A – No, we don’t coordinate benefits with Medicare advantage. No subsidy with that.
Q – What’s the rate now? Percentage towards premium?
A – Not sure of amount goes towards drugs off the top of my head. They’ll look at that Tuesday as well.
Q – Some drugs not covered under Medicare D?
A – Correct, we have our own drug formulary committee that decides, and the board decides what makes the final cut of what drugs we cover on our plan, how we cover them and the ones we don’t. If you go to part D, the plan doesn’t have any control, or any say over what those plans cover and what they don’t, they’re their own separate entities. We cover I know, but I can’t tell you if a part D would in the future or not.
With our plan we don’t cover everything or else the plan would be bankrupt, we do send a letter of medical necessity and can appeal to have certain drugs covered in certain situations. With generics, and this gentleman was asking me about new generics, especially if they’re brand new generics – we don’t set drug prices at EBD, that’s all done through the drug companies, so you have a new generic come out, it is going to be the same price as the brand name one for a while, then after a while it falls and that’s when you can change what tier the meds are in. Our plan does try to be as generic as possible and if it’s a generic that’s approved by the FDA, it is required to have the exact same chemical makeup and effects of that brand name drug, the only difference may be the appearance/logo or color. We are now to over 90% generic use, which does help when those prices fall, so everyone saves money.
If we’re not covering drugs you have been prescribed, again we have an appeals process but if they’ve excluded a drug already, then that kind of limits your appeal process, but if it’s a brand-new drug, one we just don’t cover, or haven’t reviewed yet, contact EBD. They do an evidence-based review and study how that drug compares to drugs we already cover. Cost comes into play, but usually they’ll go after the benefits that are not being offered through our drugs right now when they’re making those decisions.
Q – Saw a program about a woman in Montana represented the state employees and went in and did a lot of research about their drug and med program, not sure what she did, but she lowered their rates big time, even contracted out of Canada, to lower the cost. Considered that?
A – Not sure about contracting programs out of Canada, I know the committee works to save as much money as they can. We have dropped them a lot. Always looking to drive down Rx costs.
We will look into it (was on 60 minutes).
Q – What if no plan changes are made?
A – If no plan changes are made, if it was last month’s board meeting, it would be a 16.6% increase. They can put more towards employees’ side or across the board, but that was last months, started in March at 27%, and it could be even lower than 16%. With deductible change, it could be 12%. Actuaries try to make predictions as close to accurate as possible but are projecting through next year. They do an average of 5% of med and pharm. Downside is if you put it off, the percentage is higher.
End of questions. Meeting adjourned.